Gasherbrum I Acclimatization Strategy: Comprehensive High Altitude Climbing Preparation
Climbing Gasherbrum I, one of the highest peaks in the Karakoram range, requires meticulous preparation, particularly regarding acclimatization. This process is crucial for climbers to adapt to the reduced oxygen levels at high altitudes, which can significantly impact their performance and safety. In this article, we will explore the physiological effects of high altitude on climbers, the recommended acclimatization timeline, prevention strategies for altitude sickness, essential gear, and effective expedition planning. By understanding these elements, climbers can enhance their chances of a successful ascent while minimizing risks associated with altitude sickness.
What Are the Physiological Effects of High Altitude on Climbers?
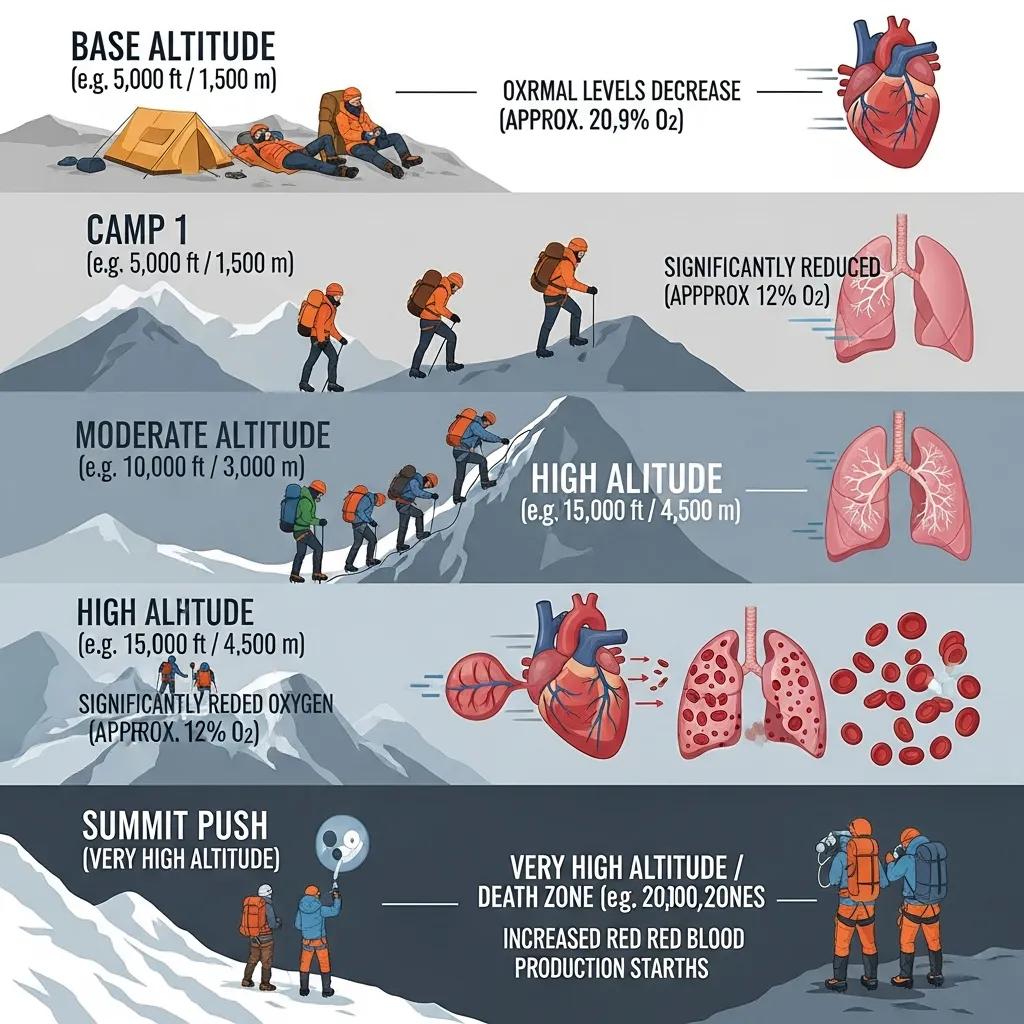
High altitude significantly affects climbers’ physiology, primarily due to the reduced availability of oxygen. As altitude increases, the atmospheric pressure decreases, leading to lower oxygen levels in the air. This reduction can result in various physiological responses, including increased heart rate, elevated breathing rates, and changes in blood chemistry. The body attempts to compensate for the lack of oxygen by producing more red blood cells, a process known as erythropoiesis. However, this adaptation takes time, which is why acclimatization is essential for climbers aiming to reach the summit of Gasherbrum I.
Further research into high-altitude physiology, such as studies on Gasherbrum II, provides additional context on how the body adapts to hypoxic conditions.
Gasherbrum II Acclimatization Adaptations & Hypoxia Performance
Additionally, the ¦E data from the same testing protocol were used for estimating Ventilatory. More precisely, the acclimatization adaptations were more enhanced during Gasherbrum II.
…
EFFECTS OF HIGH–ALTITUDE ALPINISTIC EXPEDITION MAY BE LESS STRONG STIMULUS FOR PERFORMANCE IN HYPOXIA, THAN ACCLIMATIZATION, 2012
The symptoms of altitude sickness can manifest as headaches, nausea, dizziness, and fatigue. These symptoms can escalate to more severe conditions, such as High Altitude Pulmonary Edema (HAPE) or High Altitude Cerebral Edema (HACE), which can be life-threatening. Understanding these physiological effects underscores the importance of a well-structured acclimatization strategy to ensure climbers can safely navigate the challenges posed by high altitudes.
What Is the Recommended Acclimatization Timeline for Gasherbrum I?

A well-planned acclimatization timeline is crucial for climbers preparing for Gasherbrum I. Typically, a 4-6 week acclimatization schedule is recommended to allow the body to adapt adequately to high altitude. This timeline should include gradual ascent techniques, where climbers increase their altitude slowly, allowing their bodies to adjust to the decreasing oxygen levels.
How to Structure a 4-6 Week Acclimatization Schedule for Optimal Adaptation?
To optimize acclimatization, climbers should follow a structured weekly plan that includes specific activities aimed at enhancing their adaptation to high altitudes. Here’s a suggested breakdown:
- Weeks 1-2: Begin with moderate ascents to base camp, focusing on hydration and nutrition. Incorporate light physical activities to stimulate cardiovascular adaptation.
- Weeks 3-4: Gradually increase altitude by ascending to higher camps, ensuring to include rest days to allow for recovery. Monitor symptoms of altitude sickness closely.
- Weeks 5-6: Conduct acclimatization climbs to higher altitudes, utilizing supplemental oxygen if necessary. This phase is critical for preparing for the summit push.
This gradual approach helps climbers build endurance and reduces the risk of altitude sickness, making it a vital component of any successful expedition.
When and How Should Supplemental Oxygen Be Integrated?
Supplemental oxygen can be a crucial tool for climbers on Gasherbrum I, especially during the final ascent. It is generally recommended to integrate supplemental oxygen when reaching altitudes above 7,000 meters, where the oxygen levels are significantly lower. Climbers should discuss their oxygen strategy with expedition operators, considering factors such as individual acclimatization rates and overall health.
Using supplemental oxygen can help alleviate the symptoms of altitude sickness and improve performance during critical phases of the climb. However, it is essential to use it judiciously, as reliance on supplemental oxygen can hinder the body’s natural acclimatization process.
How Can Altitude Sickness Be Prevented During Gasherbrum I Expeditions?

Preventing altitude sickness is paramount for climbers on Gasherbrum I. The key strategies include gradual ascent, maintaining proper hydration, and monitoring symptoms closely. Climbers should be aware of their bodies and recognize early signs of altitude sickness to take appropriate action.
What Safety Protocols and Monitoring Techniques Are Essential?
Implementing safety protocols is essential for managing the risks associated with altitude sickness. Climbers should:
- Monitor Symptoms: Regularly assess for symptoms of altitude sickness, such as headaches, nausea, and fatigue.
- Emergency Preparedness: Have a clear plan for descending to lower altitudes if symptoms worsen.
- Hydration and Nutrition: Maintain adequate hydration and consume high-calorie foods to support energy levels.
These protocols can significantly enhance safety during the expedition, ensuring that climbers are prepared to respond to altitude-related challenges.
Which Medications and Natural Remedies Support Prevention?
Several medications and natural remedies can support the prevention of altitude sickness. Commonly used medications include Acetazolamide, which helps speed up acclimatization by promoting respiratory alkalosis. Additionally, natural remedies such as ginger and ginseng may help alleviate nausea and improve overall well-being. Staying hydrated is also crucial, as dehydration can exacerbate symptoms of altitude sickness.
The effectiveness of medications like Acetazolamide in preventing acute mountain sickness and aiding acclimatization has been a subject of detailed study.
Acetazolamide Efficacy for AMS Prophylaxis & Acclimatization
efficacy of acetazolamide for the prophylaxis of AMS and disclose potential factors that affect the treatment effect of acetazolamide and body mass, height, degree of prior acclimatization.
Efficacy of acetazolamide for the prophylaxis of acute mountain sickness: A systematic review, meta-analysis and trial sequential analysis of randomized clinical trials, 2021
What Gear Is Essential for Effective Acclimatization on Gasherbrum I?
Having the right gear is vital for climbers preparing for Gasherbrum I. Essential gear includes high-quality climbing equipment, appropriate clothing layers, and safety equipment designed for extreme conditions.
To ensure you have all the necessary equipment for your climb, consider consulting gear and safety guidelines. Proper preparation is key to a successful and safe expedition.
How to Choose and Use Acclimatization-Specific Gear?
When selecting gear for acclimatization, climbers should consider the following:
- Climbing Gear Essentials: Invest in high-altitude boots, crampons, and ice axes that are reliable and suited for the terrain.
- Clothing Layers: Use a layering system that allows for temperature regulation, including moisture-wicking base layers, insulating mid-layers, and waterproof outer layers.
- Safety Equipment: Ensure that safety gear, such as helmets and harnesses, is in good condition and suitable for high-altitude climbing.
Proper gear selection and usage can significantly enhance climbers’ comfort and safety during their acclimatization process.
How Should Climbers Plan Their Gasherbrum I Expedition for Successful Acclimatization?
Effective expedition planning is crucial for successful acclimatization on Gasherbrum I. Climbers must consider various factors, including itinerary planning, logistical support, and risk management.
For those looking to plan their next adventure, trip planning is essential. A well-thought-out plan can make all the difference in ensuring a safe and enjoyable experience.
What Are Key Considerations in Trip Planning and Logistics?
When planning an expedition, climbers should focus on:
- Acclimatization Strategy: Develop a clear acclimatization plan that includes gradual ascents and rest days.
- Training Regimen: Prepare physically through a structured training program that enhances endurance and strength.
- Emergency Preparedness: Have contingency plans in place for emergencies, including evacuation routes and communication strategies.
These considerations are essential for ensuring a well-organized and safe climbing experience.
How to Integrate Acclimatization Strategy into Overall Climbing Plan?
Integrating acclimatization strategies into the overall climbing plan involves:
- Structured Acclimatization Plan: Ensure that the acclimatization schedule is aligned with the climbing itinerary.
- Rest Days Importance: Schedule adequate rest days to allow for recovery and adaptation.
- Monitoring Physical Conditions: Regularly assess climbers’ physical conditions to adjust the plan as needed.
This integration is vital for maximizing the chances of a successful summit while minimizing the risks associated with altitude sickness.
What Can Be Learned from Recent Gasherbrum I Expedition Case Studies?
Recent expeditions to Gasherbrum I have provided valuable insights into effective acclimatization strategies and the challenges climbers face at high altitudes. Analyzing these case studies can inform best practices for future climbers.
How Have 2023-2026 Expeditions Informed Acclimatization Best Practices?
Expeditions conducted between 2023 and 2026 have highlighted the importance of staged acclimatization and the use of supplemental oxygen. Climbers have reported that gradual ascents, combined with strategic rest days, significantly reduce the incidence of altitude sickness. Additionally, the integration of technology, such as wearable devices for monitoring vital signs, has emerged as a valuable tool for enhancing safety during climbs.
What Innovations in Acclimatization and Safety Have Emerged?
Innovations in climbing safety and acclimatization strategies have also emerged from recent expeditions. New safety protocols, including enhanced communication systems and real-time health monitoring, have been developed to improve climber safety. Furthermore, advancements in climbing gear, such as lightweight and insulated equipment, have made high-altitude climbing more accessible and safer.
How Does Gasherbrum I Acclimatization Compare to K2 and Other Himalayan Peaks?
Understanding how acclimatization strategies for Gasherbrum I compare to those for K2 and other Himalayan peaks can provide valuable insights for climbers.
What Are Similarities and Differences in Acclimatization Strategies?
Both Gasherbrum I and K2 require similar acclimatization strategies, emphasizing gradual ascent and the importance of rest days. However, K2 presents unique challenges due to its technical climbing routes and higher altitude, necessitating a more rigorous acclimatization schedule. Climbers on K2 often face harsher weather conditions, which can further complicate the acclimatization process.
How Can Lessons from K2 Enhance Gasherbrum I Preparation?
Lessons learned from K2 expeditions can enhance preparation for Gasherbrum I by emphasizing the need for thorough training and preparation. Climbers can benefit from adopting K2’s rigorous acclimatization protocols, including the use of supplemental oxygen and advanced safety measures. By applying these lessons, climbers can improve their chances of success on Gasherbrum I.
What Frequently Asked Questions Do Climbers Have About Gasherbrum I Acclimatization?
Climbers often have questions regarding the best practices for acclimatization on Gasherbrum I, particularly concerning altitude sickness prevention and the acclimatization timeline.
What Is the Best Way to Prevent Altitude Sickness on Gasherbrum I?
The best way to prevent altitude sickness on Gasherbrum I is through gradual ascent, proper hydration, and monitoring for symptoms. Climbers should ascend slowly, allowing their bodies to adapt to the changing altitude, and stay hydrated to support overall health.
How Long Does Acclimatization Typically Take for Gasherbrum I Climbers?
Acclimatization for climbers on Gasherbrum I typically takes 4-6 weeks, depending on individual responses to altitude and the specific acclimatization strategies employed. Factors such as fitness level, previous high-altitude experience, and overall health can influence the duration of acclimatization.
For more information on planning your next climb, visit Global Summit Guide.